LOW BACK PAIN
 “I have arthritis of the back”
“I have arthritis of the back”
“I have sciatica”
“I have spinal stenosis”
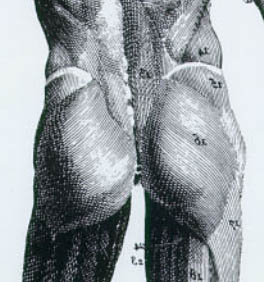
ANATOMY: The figure shows the sources of low back pain and related disorders.
PERSPECTIVE
Low back pain ranks with cardiovascular diseases and mental illnesses as the major causes of the escalation of healthcare costs.
The fact is there is no distinct boundary between the above disorders. The muscles, joints and nerves constitute the largest system affecting people’s health and productivity. As a dominant system, it also plays a role in the genesis and perpetuation of or prevention of and recovery from common diseases and disorders of other organs such as obesity, cardiovascular diseases such as high blood pressure and cholesterol, heart diseases, stroke, diabetes, psychiatric illnesses, osteoporosis and related complications, etc.
This prevalent problem is significant in light of the fact that individuals afflicted with LBP suffer and endure needlessly the pain, suffering and disability. Their families, friends and employers share their emotional anguish and financial strain.
FACTS
The profile of low back pain including leg pain, ache, sciatica, weakness, abnormal sensations such as tingling, numbness and pins and needles, muscle spasm and stiffness, joint swelling and stiffness (LBP) comprises:
- LBP is a common affliction of people especially in the industrialized nations in America, Europe and Asia.
- It is estimated that 80 – 95% of the population is afflicted by LBP in their lifetime. The fact is LBP and its chronic sequalae afflict all humans.
- It is the most common cause of disability in America for individuals less than fifty years old.
- The degeneration, spinal stenosis (narrowing of the canal, foramina or channels for the spinal cord and lumbosacral nerves), leg weakness and disability in seniors are the inevitable consequences of poor management of LBP.
- Lack of proper and delayed diagnosis and ineffective and improper treatments cause pain, suffering, increased morbidity and mortality in people.
- Since LBP is a multi-facet problem, disorder, disease, ailment, any program comprising only individual physician, doctor or therapist is ineffective to manage LBP.
PERPLEXION
As a common, prevalent and costly affliction affecting all people, there was no concerted and universal effort heretofore made to communicate vital information in the prevention, care and management of low back pain and related disorders. Patients are inundated with inaccurate information. Moreover, information being passed on to the patients may neither address the problem nor base on fact. Consequently, many individuals suffering from the above are misguided.
- Useful and intelligent information is not readily available to individuals with LBP.
- Patients are deluged and confounded by opinions, advises, prescriptions, tests, treatments and procedures – effective or otherwise.
- Money is spent and wasted as patients continue to buy and consume services, products, devices, remedies and drugs that may be useful, useless or, in many instances, even harmful.
- Costly tests such as MRI, CTScan and electrodiagnosis (EMG/NCV) often add more confusion, dismay and anxiety.
- After the time for healing has been used and treatments have failed to decrease the pain, suffering and disability, the patients with chronic disabling LBP drift toward ineffective or unnecessary procedures including surgery.
- Desperate, confuse, naïve and vulnerable patients may have to make a difficult and crucial decision to proceed with ineffective or unnecessary procedures including surgery.
- Essentially, most back surgeries are the poor alternative to the effective management of LBP.
- Failed back and recurrent LBP and related complications and consequences after surgery are extremely common.
- Repeat surgeries may be recommended and performed with same consequences.
ESCALATING HEALTHCARE COSTS
- In America, people, employers, companies, corporations and third-party payers are spending billions of dollars every year on unnecessary tests and ineffective treatments, therapies, care and drugs relating to LBP.
- Absenteeism, lost wages and productivity are extremely costly to people, companies and corporations.
- The liabilities and insurance and workers’ compensation costs continue to escalate. The solution to the above problems was heretofore not in sight.
LOW BACK PAIN IN THE NUTSHELL
The following information helps people to:
- Understand the importance of caring for their backs.
- Avoid the pitfalls in their searches for the proper care and treatments of LBP.
- Exercise some control on the decision-making process.
- Undertake appropriate responses in consultations with their physicians.
The low back is the conduit for sensory, motor and autonomic nerves shuttling the life force between the spinal cord and the abdominal and pelvic organs, muscles and joints in the legs.
The vital structures of the low back comprise:
- Ligaments
- Low back muscles and tendons
- Leg muscles and tendons
- Trigger points and fibromyalgia
- Facets
- Joints
- Fasciae
- Spinal vertebral bones
- Intervertebral discs
- Spinal cord in the spinal canal
- Nerve roots in the spinal canal
- Nerve roots in the intervertebral foramina
- Nerves
- Dura mater covering the spinal cord and nerve roots
- Neuronal circuitry with reference to:
- Sciatic and referred pain in the legs
- Abnormal sensations such as numbness, tingling, pins and needles
- Myofascial pain syndrome
- Arteries
- Veins
- Lymphatic channels
Essentially, the vital structures of the low back influence the well-being of an individual. They regulate the functions and affect the health of the abdominal and pelvic organs and muscles, joints and bones of the legs. The strength of the legs for walking and mobility is vital to all humans. They play a vital role in the genesis and perpetuation of or prevention of and recovery from common diseases and disorders of other organs such as obesity, high blood pressure and cholesterol, heart diseases, diabetes and related complications. In other words, the health and longevity of an individual can be secured by a healthy low back.
Unlike other body parts, the low back also cushions the weight of the upper body. It absorbs the impact when the feet or buttocks absorb the forces from the ground or surfaces. As a person bends, twists, walks, runs or performs the activities of daily living, fluctuating gravitational and muscular forces are imposed on the low back. Therefore, the back muscles, joints, nerves, tendons, ligaments, discs and bones – the tissues – are constantly subjected to varying strains and, in certain settings, they can be sprained and injured leading to inflammations and pain.
In a person’s life, the natural course of LBP is the hurt and then spontaneous recovery without intervention. For example, LBP in a well-known weekend sports enthusiast in balmy sunny weather and a home laborer – shoveling snow, raking leaves, picking grocery or a child, moving of furniture, dancing, etc. It was said that most LBP resolves within one week to several weeks and, in these circumstances, the tissues are able to spontaneously recuperate, repair and heal without the interventions.
However, there are common LBP in which the tissues cannot recover or the strain and sprain are too great to result in the spontaneous resolution of the inflammation and pain. Consequently, LBP can cause varying degrees of loss of activities of living, function and disability. LBP which does not spontaneously resolve necessitates the person to seek treatments. Treatments bring relief, recovery, restoration of function, and affect the course and outcomes of LBP.
Common symptoms and complaints
General constitution: fatigue, malaise, poor or disrupted sleeps and insomnia.
Quality of pains: sharp, piercing, lancinating, knife-like, sciatica, shooting, electricity, radiating, soreness, burning, hot-iron, dull, ache, cramps, gnawing, depressing, unbearable, sickening and nauseating.
Quality of sensations:– agony, numbness, sciatica, paresthesia, tingling, pins and needles, running water, ants crawling, decreased light touch, pin pricks and loss of sensations.
Leg, foot and toes: stiff, rigid, heaviness, swelling, “not my leg or foot”, weakness, knee buckling or locking, restless, unsteadiness, shuffling, slapping foot, walking difficulty, gait disturbances and fallings.
Gastrointestinal: loss of appetite, upset stomach, indigestion, gas, bloating, poor intestinal motility, irritable bowel syndrome, constipation and diarrhea.
Urinary: urinary retentions, poor control of urine and increased urinary frequency. Biomechanical disorders comprise stress, strain and sprain of the soft tissues such as the ligaments, muscles and bones of the low back. They are the most common cause of inflammation, pain, muscle stiffness and spasm and loss of mobility of the low back. These frequently occur in people in their ordinary activities of daily living.
Like the knee joint, the mobility such as bending, twisting and turning of the back is possible because of multiple small joints and facets, the short and long ligaments and muscles. These facets and joints are held together and supported by the ligaments, muscles and their tendons. Tremendous pressure and forces are constantly put on these structures.
A weakness or imbalance of these structures leads to the stress, strain or sprain of the ligaments, muscles, tendons, joints and facets. In most common LBP, usually, a group of related structures such as the ligaments, muscles and joints are stressed or strained at a time. Thus, people with LBP cannot exactly isolate or pinpoint the structure or structures involved in LBP.
In young individuals, most LBP is perceived to localize to back muscle ache and stiffness. In most instances, the structures have the resiliency to repair, recuperate and recover from the stress, strain or injury. This is a reason why most common LBP spontaneously resolves within one week to several weeks without any medical intervention.
However, when the ligaments, muscles, tendons, joints and facets are inflamed, LBP is experienced as ache and pain, muscle stiffness, spasm, rigidity, weakness of the back causing the loss of mobility of the back. Oral medications usually yield relief and hasten the recovery process.
On the contrary, the degenerative process progresses in older individuals leading to the degeneration and aging of the above soft tissues. Inevitably, arthritis, facet osteoarthritis, weak ligaments, muscles and tendons and vertebral bone and disc occur. These structures are less supported by the weakened ligaments, muscles and tendons in the face of perpetual pressure and forces. These structures are prone or more susceptible to stress, strain and injuries, however minor, and inflammation and pain. Consequently, LBP and related widespread and complex disorders become more prevalent and common. The range of motion and mobility of the spine are decreased. Deformity of the low back such as spinal stenosis (narrowing of the channels for the nerves and spinal cord) and shifting of the spine ensue. In these instances, people are less likely to recover from LBP even with most medical interventions.
In these individuals, the results are recurrent and disabling back pain involving arthritis, facet osteoarthritis, arthropathy, joint pain, weak and inflamed ligaments, muscles and tendons. The weakened structures further cause a constellation of widespread low back and leg pain, symptoms and disorders, visceral and pelvic organs disturbances and diseases. Myofascial pain syndrome or fibromyalgia afflicts all people and is as common and prevalent as back pain. Detailed information is in Enigma Unraveled.

In the figure, each dot or pox is a trigger point in the myofascial pain syndrome.
For the complete view and the anterior view showing more trigger points relating to the back, please go to Patient Page.
Each sacroiliac joint is a gray dot next to the midline, at the end of the iliac bone crest represents by a curve white line above each buttock.
Essentially, myofascial pain syndrome or fibromyalgia is mediated and propagated by the sensory and autonomic nervous systems. It comprises inflamed and hyperirritable nerve endings, muscles, tendons, bursae and fasciae also commonly known as trigger points or acupuncture points, fibrositis, myofascial pain, tendonitis, bursitis and fasciitis.
Myofascial pain syndrome causes a widespread and complex pain, symptoms, conplaints and disorders such as varying degrees of sharp, lancinating, dull, achy, burning, throbbing and miserable pains, weakness and abnormal or unpleasant sensations such as tingling, pins and needles and numbness in the back and legs. Patients often cannot lie on the pain side of the body. Weakness or heaviness the leg causes fallings. Swelling of the back and legs, poor or disrupted sleep, gastrointestinal and pelvic disorders are common.
Sacroiliitis is the inflammation and pain of the sacroiliac joint – see the above figure. It is common and prevalent and closely associated with LBP.
The sacroiliac joints (SI joints) are easily seen in the back of a slender person as two dimples on the skin just above the buttocks. The SI joints are on both sides of the spine and are the links between the spine and the pelvis. These joints are supported by strong ligaments, muscles and tendons binding the spine to the pelvis. They bear all the weight of the body above them and sustain the load and pressure put upon them when a person is upright, stands, walks, runs or jumps.
Injury, inflammation and pain of the SI joints are common and prevalent. They are commonly associated with the inflammation and disorders of the above back structures.
They are also commonly stressed and strained in the activities of daily living such as walking, bending and lifting. They are more prone to injuries when the ligaments are lax, the muscles and tendons are weak, stiff or not resilient, muscular imbalances and misalignment of the body.
Other stress and strain of the SI joints can be caused by excessive force acting on them such as in heavy or prolonged lifting, bending of the trunk, torsional strain, movement from stoop to stand and falling on the buttocks. Certain activities in sports such as skiing, snowboarding, golfing, bowling, running and motor vehicle accident can also cause injury to the SI joints.
In the above conditions, walking, standing, trunk movements and even lying down cause pain, muscle stiffness and painful spasm in the back above the buttock of the involved side. Pain can radiate into the buttock and leg. Leg muscles can also become stiff and spastic. Movements and mobility become restricted.
Herniated disk (nucleus pulposus) is involved in the inflammation and pain of the back soft tissues such as joints, ligaments, fasciae, tendons, muscles and nerves. Disc bulging or disc herniation is commonly associated with low back and leg pain.
Disc Herniation described the roles of the vital structures of the low back spine in the causations of symptoms and manifestations of low back and leg pain, abnormal sensations in the leg and related disorders. It defines and discusses the relationship between the above pain, symptoms and disorders and the MRI and CTScan findings of the disc.
It also notes that disc bulges and herniation are observed in people who have no low back and leg pain and symptoms. In other words, despite popular belief, in many settings, a herniated disc does not cause low back pain and related symptoms and manifestations.
Coccygodynia is the inflammation and pain in the tail bone. The pain can radiate up the lower sacrum or down into the genital area. It is usually caused by a fall in a sitting position or direct injury to the tail bone, poor sitting posture or poorly designed chair. The inflammations and pain are also caused by stress, strain or sprain of the sacrococcygeal ligament holding the tail bone to the sacrum or a fracture of the tail bone.
Trauma and injuries are not uncommon to the spine, spinal cord, linings of the spinal cord and nerve. Most of the trauma and injuries are minor and inflammations and pain eventually resolve. However, more serious injuries can occur such as hyperextension (bending backward) injury of the low back, overflexion (bending forward) of the low back or sprung back such as in motor vehicle, motorcycle, bicycle and ski accidents.
Non-mechanical causes of low back pain and inflammations are less common. However, LBP can herald in many diseases. Symptoms and manifestations include acute (happen suddenly), recurring, extraordinary amount of pain, stiffness and muscular spasm and dysfunction of the low back. Symptoms and disorders in other parts of the body include abnormal bowel sensations and movements and urination, cramps and ache in the leg(s) and foot/feet, weakness of the leg(s) and foot or feet, tingling, numbness and abnormal sensations of the leg(s) and foot or feet including toes.
Referred pain is caused by a disorder or pain of a part of the body. The pain is referred to and perceived in another distant part of the body that is not directly affected by the cause of the disorder or pain.
Most common sources of referred pain to the low back are the organs in the abdomen, pelvis and retroperitoneal space (an area in the back of the abdomen) such as stomach, intestines, uterus and ovaries, and kidneys. For example, pain of peptic ulcer, diverticulitis of the colon, pelvic inflammatory disease, acute prostatis, trochanteric bursitis (inflammation of the bursa of the hip area) and pain during menstruation can refer pain to the low back.
Infections are caused by bacterias, viruses, fungi and parasites. These organisms can reach and infect the spine, intervertebral bone and disk and the epidural (lining of the spine) space.
Abscess is caused by an infection by the above organisms of the spine, intervertebral bone and disk and the epidural space.
Cancers comprise local primary cancer affecting the vertebral bone of the spine, lining of the spinal cord and nerves such as prostatic cancer, plasmacytoma, chordoma, chondrosarcoma, fibrosarcoma, multiple myeloma, osteoma, neurofibroma and ependymoma.
Cancers comprise metastatic cancers spreading from other organs of the body such as breast, lung, prostate, kidney, thyroid, liver and large intestine.
Inflammation comprises ankylosing spondylitis, arachnoiditis (inflammation of the web-like lining of the spinal cord), herpes zoster from chicken-pox virus.
Metabolic and vascular diseases comprise osteoporosis, diseases of the bone such as Paget’s disease, hyperparathyroidism (over-active parathyroid glands), Fanconi’s syndrome, renal osteodystrophy and disorders of the aorta (see below).
Rheumatism comprises gout, spondylarthropathies and Familial Mediterranean Fever.
Cardiovascular diseases comprise aortic aneurysm, infarction (loss of blood supply to the nerves) and hematoma.
Neuropathy comprises diseases of the nerve caused by diseases such as diabetes, cancers and alcohol that affect the nerves of the low back.
THE MOST EFFECTIVE MANAGEMENT OF LBP
CAUTION: You must consult and see physicians skilled in the diagnosis and treatment of back pain and related disorders (LBP). The information herein and related work only serve to inform and nothing more.
- Delayed seeing, diagnosis and proper treatment of LBP by competent physicians pose an increase risk and complication of an illness which can become a life-or-death matter.
- LBP is extremely complex, insidious and can be serious.
- Some causes of low back pain:
- Degeneration, Rheumatologic Diseases, Trauma & Others
- Metabolic Bone Diseases
- Infections
- Cancers
- Blood Vessel Diseases
- Psychogenic & Psychosomatic Disorders
The means for preventing and treating LBP and the means for realistically curbing the escalating healthcare costs can only be effectively applied in a team approach comprising:
- Well-informed, educated and compliant patients.
- Skilled physicians, massage therapists and exercise physiologists.
Well-informed, educated and compliant patient plays a crucial role in the management of his or her LBP. Patient can give accurate and reliable history including the cause, assist in the physical examination and, of course, complying with the care, treatments and management LBP. Ultimately, patient decides the outcomes of a good program of care and management of LBP.
The clinicians are endowed with different skills and varying and diverse abilities and expertises to treat and care for low back pain and related disorders. The cornerstone of the effective management of LBP comprises:
- The effective ongoing program of maintaining the health and optimal condition of the lumbosacral spine.
- Education, constant reinforcements and compliance being performed and concerted efforts of patients themselves.
- The biomechanics of the lumbosacral spine.
- The expeditious and effective diagnosis, treatments, whenever necessary and indicated, and support by skilled and knowledgeable physicians and therapists.
In tens of thousands of patient cases particularly those in seniors, the spine and legs served as the crucible for the data supporting the current medical approach.
Diagnostician is king, expert is emperor
The effective management of LBP is complex and requires skilled physicians with expertise in many disciplines. Expert, not unlike an Emperor ruling a far-flung empire, has the experience and skill to recognize the simplicity and complexity of LBP and can choose and tailor the treatments and management suitable for LBP of an individual. A physician’s accurate diagnosis leading to the effective care, treatments and management result in the good outcomes. A skilled physician with excellent knowledge of human anatomy expertly performs the treatments resulting in fast and early recovery.
Effective treatments
Always consult your physicians before acupuncture medicine to determine if acupuncture medicine is the appropriate treatment or the treatment of choice.
Acupuncture Medicine is scientifically supported by several recent scientific studies, numerous clinical reports and the extensive researches performed by this writer. With correct diagnosis by a physician, acupuncture is very effective, if not the most effective, anti-inflammatory electro-therapeutics for treating acute and chronic low back pain and related disorders.
Aside from the above, acupuncture medicine is an excellent anti-inflammatory therapeutics in lieu of oral and injectable drugs such as the nonsteroidal anti-inflammatory drugs (NSAIDS) such as ibuprofen, naprosyn and ketolorac and the steroids such as prednisone. In many of the above LBP and settings, LBP and related disorders are not responsive to oral or injectable drugs.
Moreover, most seniors and some people have the following concerns:
- Risks of gastrointestinal irritation and bleeding
- Intolerable or adverse side effects such as vomiting, dizziness and weakness
- Drug allergy
- Drugs adverse interaction
- Ineffectiveness of the medications
- Appropriate care in lieu of surgery
- Surgery is not an option
In the hands of a skilled physician who is an expert in human anatomy, acupuncture medicine is very safe and almost always painless. The relief from LBP and related disorders may be immediate.
Trigger point injection in myofascial pain syndrome is performed by many skilled physicians throughout America. This routine procedure involves the use of a small and thin needle to safely inject a small quantity of local anesthetics such as lidocaine solution into the painful trigger point or site. In the hands of the skilled physician, the trigger point injection is very safe and almost always painless. The resolution of pain and associate symptoms may be fast and remarkable.
Similarly, tendonitis, bursitis and fasciitis can also be treated by local anesthetics to obtain similar relief.
Acupuncture medicine and local anesthetics are synergistic in action. In other words, both give relief from pain and associate disorders.
Oral medications comprise various medications that are used singly or in combination. A physician’s accurate identification of the sources and causes of LBP and the diagnosis allow the efficacious use of medications resulting in corresponding response and the relief from LBP, the improvement of the function and speed up recovery.
Nonsteroidal Anti-Inflammatory Drugs (NSAIDS) are the most commonly prescribed and consumed by patients with LBP. Some common drugs are Aspirin, Motrin, Naprosyn, Relafen, Daypro, Celebrex, Dolobid, Trilisate, Ansaid, Daypro, Indocin, Clinoril, Lodine, Feldene and Toradol. A common side effect is irritation and pain of the stomach.
Acetominophen or Tylenol is used with varying success and degrees of relief. Long-term use can cause liver toxicity.
In certain circumstances, the muscle analgesics and relaxants are used with varying success and degree of relief. Soma, Parafon Forte, Flexeril, Robaxin and Valium are common drugs. Side effects include drowsiness and weakness which are not well tolerated especially by seniors.
Narcotic analgesics are used with varying success and degrees of relief. Codeine and percocet are the two common painkillers. Side effects such as drowsiness and weakness are not well tolerated especially by seniors. Furthermore, the limitation to use is the anxiety of patients and physician of the tendency to the drug addiction.
Antidepressants in low doses can be used for management of LBP. Amitriptyline, Nortriptyline and Desipramine are some of the commonly used drugs. Side effects such as drowsiness and weakness are not well tolerated especially by seniors.
Steroids by mouth or by injection such as prednisone are commonly used. The limitation is the side effects on the natural hormones of the body and body metabolism. In most LBP, epidural steroids comprising the injection of steroids into the epidural space of the spinal cord are ineffective. However, a skilled physician can usually determine the type of LBP and related disorders that may be responsive to epidural steroids.
Massage therapy
As a team member, a skilled massage therapist can identify and treat the musculoskeletal spasm, stiffness and contracture. Thus, a skilled massage therapist significantly contributes and effects the good outcomes in the care and treatments of LBP.
The massage therapy usually comprises the mobilization of soft tissues, release of myofascial and trigger point, stretching and balancing the muscles and tendons and the release of soft tissue contracture.
Exercise physiology
In most circumstances and settings, weak and lax ligaments, muscles and tendons contribute to the causes of LBP.
A skilled exercise physiologist as a team member with the physicians and therapists can significantly contribute and affect the good outcomes of LBP.
The exercise regimens include proper cardiovascular conditioning, muscular toning, conditioning, strengthening, toning, stretching and ergonomics of the back.
Always consult your physicians including your heart physicians before participation.
Nutrition
Obesity or excess body weight imposes stress and strain on the spine and its vital structure and contribute to the cause of LBP. In most circumstances and settings, in conjunction with the above, a balance caloric expense and intake and good nutrition ensure the health and optimal conditions of muscles, tendons, joints, nerves, and bones.
Always consult your physicians including your heart physicians before participation.
BACK PRODUCTS
Furniture such as a chair or a seat affects the posture an individual using it. Most people spend more than one third of their lives on furniture at home or work. So, the ergonomic and supporting furniture is important.
Bed affects the posture of the low back and legs of a person lying on it. A firm and supporting bed is important. Most people spend about a third of their lives on bed or the like. In general, a good bed should give a person a good night of sleep. The person – with or without LBP – should awake refreshed and have no complaint or exacerbation of LBP upon arising from the bed.
Back braces and corsets comprise various types of soft and hard braces and corsets that can be used to aid the muscles, ligaments and tendons in the support of the low back. These devices are helpful and effective during the time of LBP. There are off-the-shelf types that can be readily bought. However, custom-made braces and corsets are crafted by skilled technicians who make prosthetics and orthotics that optimally fit the contour of an individual.
A physician who treats LBP can advise the patient on the use, application and indications and the sources for acquiring the braces and corsets.
Gel supports, cushions, insoles and footwear can significantly reduce the forces being transmitted from the ground to the back as each foot of an individual strikes the ground during standing, walking, jogging or running on hard ground or concrete surfaces. Thus, these devices affect the posture of and reduce the load on the muscles, tendons, ligaments, joints, nerves, bones and disc of the back.
In the industrialized nations, in general, people walk on or pound with their feet the concrete or hard ground or surfaces such as the streets and floors in the homes or offices. Therefore, people should use these devices as the foremost, inexpensive and cost-effective passive means for reducing the load and stress on the above back structures to reduce LBP in people.
Generally, most brands of running sneakers are well designed for absorbing the impact from the ground. On the contrary, well-designed dressed shoes for absorbing the impact from the ground are uncommon.
A physician who treats LBP or some podiatrists can advise the patients on the use, applications of and indications and the sources for acquiring gel supports, cushions, insoles and footwear.
Traditional mechanical back stretcher and the like require that a stretching force of more than 50% of the body weight of the person is applied to stretch the soft tissues of the low back in order for it to be effective. In brief, at this level of force, the stretching is uncomfortable if not painful and is usually not tolerable by most patients. Therefore, essentially, this type of back stretcher is ineffective.